Updates to Treatment Protocols
- Second-Line Therapy for Bone Pain
- For patients unresponsive to bisphosphonates or those with renal insufficiency contraindicated for bisphosphonates, anti-RANKL monoclonal antibodies (e.g., denosumab) are recommended. FDA-approved biosimilars are suitable alternatives.
- Additions for Indolent and Smoldering Subtypes
- For indolent systemic mastocytosis (ISM) and smoldering systemic mastocytosis (SSM), cladribine or peginterferon alfa-2a is added as “potentially beneficial in select cases.”
- Adjustments for Aggressive Subtypes
- For aggressive systemic mastocytosis (ASM), systemic mastocytosis with associated hematologic neoplasm (SM-AHN), and mast cell leukemia (MCL) ± AHN:
- If clinical benefit fails to meet the 2013 IWG-MRT-ECNM response criteria, restage the disease, consider second-line multiagent chemotherapy, and evaluate eligibility for allogeneic hematopoietic cell transplantation (HCT).
- For aggressive systemic mastocytosis (ASM), systemic mastocytosis with associated hematologic neoplasm (SM-AHN), and mast cell leukemia (MCL) ± AHN:
- Removal of Toxicity Management Content
- Sections on avapritinib and midostaurin toxicity management were removed.
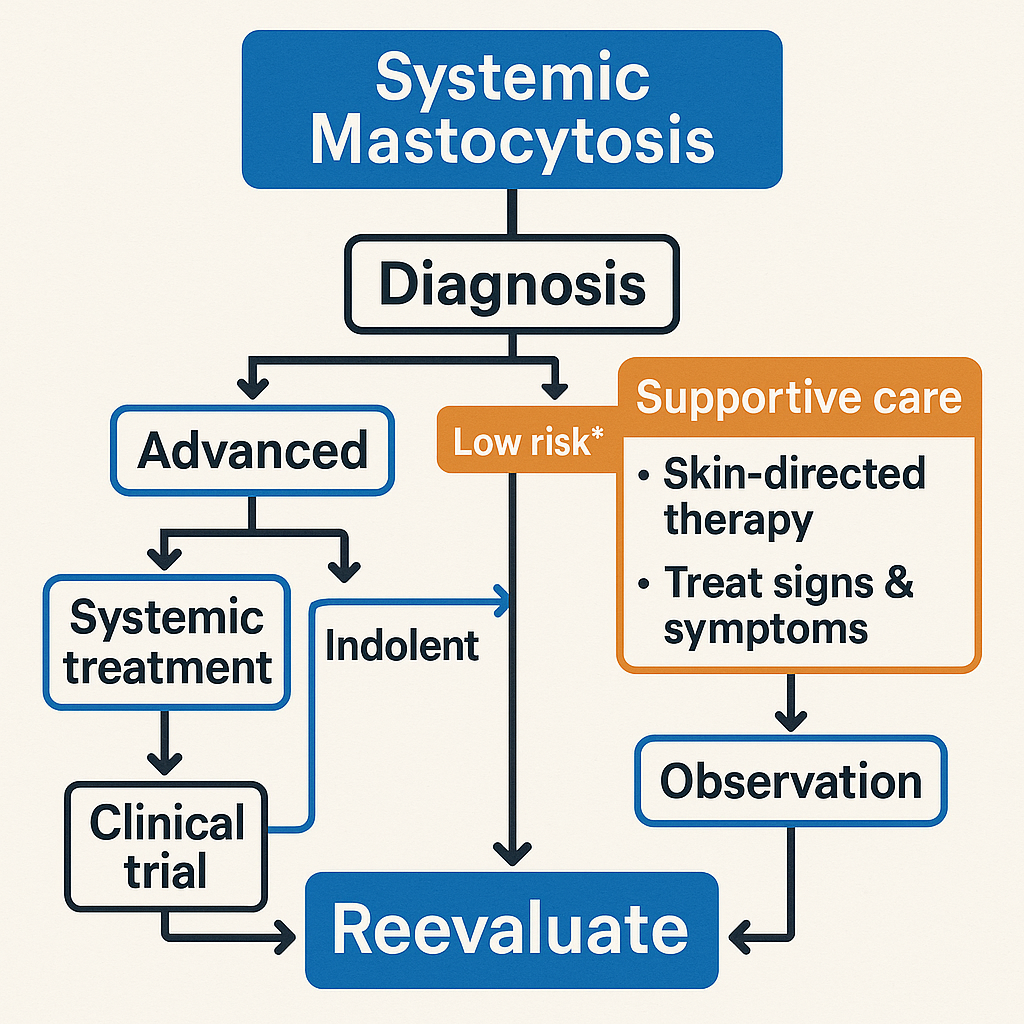
Treatment Recommendations by Subtype
- Symptomatic ISM or SSM
- First-line: Mediator-targeting therapies for symptom control; clinical trial enrollment is preferred.
- Avapritinib is recommended for symptomatic ISM patients with platelet count ≥50 × 10⁹/L.
- Cladribine or peginterferon alfa-2a may be used in severe, refractory cases with mediator-related symptoms or bone disease.
- ASM, SM-AHN (SM-dominant), and MCL (with/without AHN)
- First-line: Clinical trials, avapritinib (platelet count ≥50 × 10⁹/L), or midostaurin.
- Other options: Cladribine, peginterferon alfa-2a (± prednisone).
- Imatinib is reserved for rare cases (e.g., KIT D816V-negative/unknown ASM, FIP1L1::PDGFRA fusion-associated eosinophilia).
Drug Efficacy and Safety
- Avapritinib
- In trials: Significant reduction in total symptom score, serum tryptase, and KIT D816V allele burden after 24 weeks in moderate-severe ISM.
- ORR: 75% in advanced SM.
- Safety: Comparable grade ≥3 adverse events (AEs) to placebo (e.g., flushing, peripheral edema). Prolongs median overall survival.
- Midostaurin
- ORR: 60% in 116 advanced SM patients, consistent across subtypes.
- AEs: Low-grade nausea/vomiting/diarrhea; grade 3–4 cytopenias (neutropenia, anemia, thrombocytopenia).
- Cladribine
- ORR: 56% (ISM), 50% (ASM), 55% (SM-AHN). Reduces mast cell metabolites and marrow burden.
- AEs: Grade 3–4 lymphopenia, neutropenia, opportunistic infections.
Allogeneic Hematopoietic Cell Transplantation (HCT)
- Retrospective data (pre-KIT inhibitor era) from 57 advanced SM patients:
- ORR: 70% post-HCT.
- 3-year OS: 74% (SM-AHN), 43% (ASM), 17% (MCL).
- Key risk factor: MCL subtype predicts poor survival.
- Prospective trials are needed to clarify HCT’s role in advanced SM.
Share this content:
1 comment so far